


Non-Profit Hospitals Are Allowed to Profit
Despite what their status as non-profits indicate, health systems across the country rake in billions of dollars of profits at the expense of patients and communities.

Most hospitals in the US are classified as non-profit — specifically, 61.1% in 2020. Non-profit hospitals play a crucial role in providing care to populations of people otherwise unable to afford high healthcare costs and unable to keep for-profit providers open. Further, these institutions often serve as great grounds for training future medical professionals and pursuing medical research.
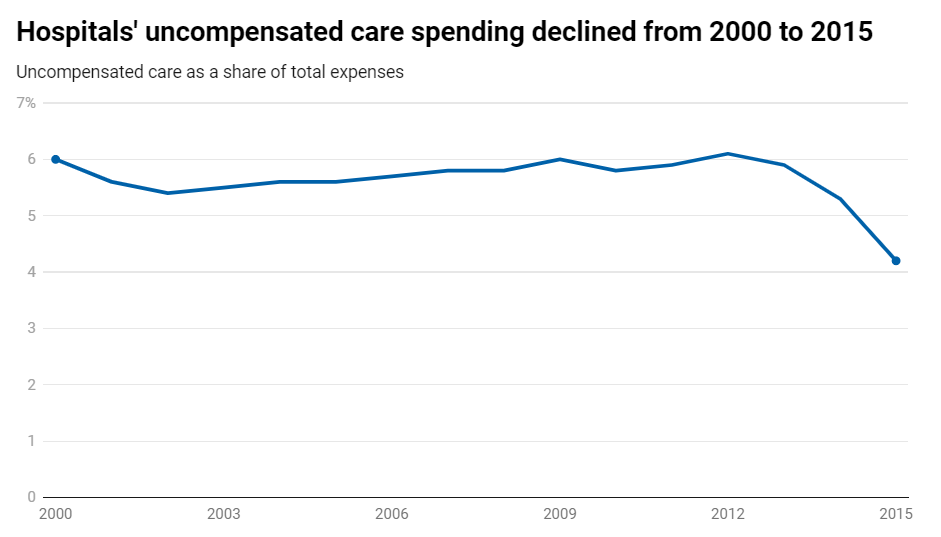
Over the past several years, however, some of these non-profit hospitals have seen profit margins raise dramatically against the backdrop of less spent providing charity care. A handful have resorted to aggressive programs to squeeze money from low-income patients whilst others have created dangerous conditions for patients by cutting staff sizes to reduce costs.
What Makes a Non-Profit
Non-profit hospitals, in the eyes of the IRS, operate as charities and face no state/local property taxes or federal income taxes. These organizations must demonstrate that they are specifically working to promote health. Not all healthcare providers are eligible for the tax exemption because they must meet the community benefit standard.
The community benefit standard assesses factors like:
Civic and community leaders being part of the governing board
Operating a full-time emergency room treating all regardless of ability to pay
Provides non-emergency care to anyone who can pay privately or through third-parties (i.e. Medicare/Medicaid)
Serves the community by providing charity care
Supports medical training and research
The specifics, of course, go more in-depth. For example, some non-profits do not need to operate emergency rooms.
How Non-Profits Behave
Non-profit hospitals technically cannot earn profits, so many use the term net income instead.
It’s not uncommon for these hospitals to have positive net incomes. These may be used for reinvestment, increased staff pay, or increased community programs like charity care.
Compared to for-profit hospitals, non-profits are more likely to have services that have lower margins like burn units and trauma care. In contrast, for-profit hospitals are more likely to have high-margin services like heart surgery.
Yet, recent trends have been at odds with the expected behaviors of non-profit hospitals. Non-profits making significant upgrades to aesthetics and otherwise nonessential amenities have been compared to hotels. It’s also no secret that executive compensation for many of these organizations can climb to millions of dollars per head per year. In 2016, seven of the 10 most profitable hospitals were non-profit.
Profit-Maximizing Practices
Some economists have speculated that non-profits have taken advantage of market power to set prices far above levels that would otherwise be justified by the cost of doing business. In one notable example, the former CEO of Mayo Clinic urged giving preference to patients with private insurance over Medicare/Medicaid because private plans tend to pay providers more than the two government health programs.
A subset of hospitals have even resorted to squeezing patients of payments even if they would otherwise qualify for charity or discounted care. One New York Times investigation of the Providence health system (51 hospitals and 900+ clinics) details a “Rev-Up” program where employees were trained to pressure patients into paying. Those who did not were hounded by debt collectors.
Although the Affordable Care Act requires non-profit hospitals to disclose financial assistance policies, there is no overarching federal rule on what the requirements for charity eligibility are. Some states have implemented their own measures, and Washington state attorney general Bob Ferguson levied a case against Providence hospitals for sending over 54,000 patients to debt collection of over 70 million dollars when they were eligible for free care.
A similar investigation of Ascension health system found that years of cutting staff to save on labor costs have triggered a nightmarish staffing crisis, especially as the COVID pandemic’s burnout led to even more physicians and nurses leaving the field. This, of course, has led to dangerous conditions for patients who are unable to receive proper attention from medical professionals. In another health system, CommonSpirit Health, a nurse was forced to call 911 to get the local fire department to help take care of patients.
In an interview with the Kitsap Sun, Central Kitsap Fire and Rescue Chief Jay Christian described the call: “The charge nurse expressed two times that they feel like they’re drowning because they had over 45 patients in the waiting room and only five nurses. She said, ‘We’re in dire straits, we need the fire department help, can somebody come up here and help us?’”
Closing the Loopholes?
One estimate finds that non-profit hospitals get more than a $60 billion tax break each year, and it seems ridiculous that some of these hospitals continue to press for higher margins at the cost of patients and the taxpayer.
To start with, tighter controls on the obligations of charity care would limit instances of poorer patients being squeezed. For example, Illinois limits the state income tax credit to the cost of free and discounted care that’s provided. States like Oregon have implemented strict rules on which patients qualify for free and discounted care.
Greater judicial authority to scrutinize non-profit hospital mergers and acquisition may provide an opportunity to rein in these hospitals on anti-trust grounds and enforce other elements of providing sufficient charity care.
Limits on debt collection practices and enforcement of surprise billing behaviors would also likely alleviate a significant headache for patients.
Potential legislation to provide the Federal Trade Commission (FTC) the power to enforce conduct may also enable better enforcement for non-profit health systems spanning multiple states.