
The Debate Around Nurse Independence
Strategies to meet healthcare provider shortages bring questions about safety

State representative Jodee Etchart (R) of Montana recently introduced Montana House Bill 313 to the floor of the state legislature, one of the latest developments in an ongoing debate on how to alleviate the healthcare professional shortage by leveraging the expertise of physician assistants (PAs) and nurse practitioners (NPs).
The Nationwide Shortage of Doctors
Even before the COVID-19 pandemic, there were widespread concerns about the availability of enough healthcare professionals in the labor market. The pandemic accelerated already concerning trends of physician burnout, and it led to a mass exodus of healthcare workers from the industry.
Consider the following quote from an advisory published by the Office of the Surgeon General
The Association of American Medical Colleges (AAMC) projected in 2020 that physician demand will continue to grow faster than supply, leading to a shortage of between 54,100 and 139,000 physicians by 2033, with the most alarming gaps in primary care and rural communities.
What’s even more concerning is how fast-approaching shortages in healthcare will disproportionately affect communities that already have difficult access to healthcare. Shortages are likely to be more extreme in low-income and rural regions where organizations have less resources to recruit and retain care providers.
Financial pressures in rural communities have been especially apparent. The same Surgeon General advisory highlighted a declining ability of rural hospitals to serve more patients:
Between January 1, 2010, and March 31, 2022, 138 rural hospitals across the nation closed completely or converted to provide services other than inpatient care. In March 2020, rural areas had between 37 and 42 percent fewer ICU beds per persons who were at risk of developing severe COVID-19 based on age and comorbidities than persons in urban areas.
Even with temporary staffing solutions, these professionals tend to cost the healthcare provider higher rates than more permanent employees. One Wyoming hospital had to stop offering labor and delivery services after a nursing shortage and the cost of temporary staffing became financially unsustainable.
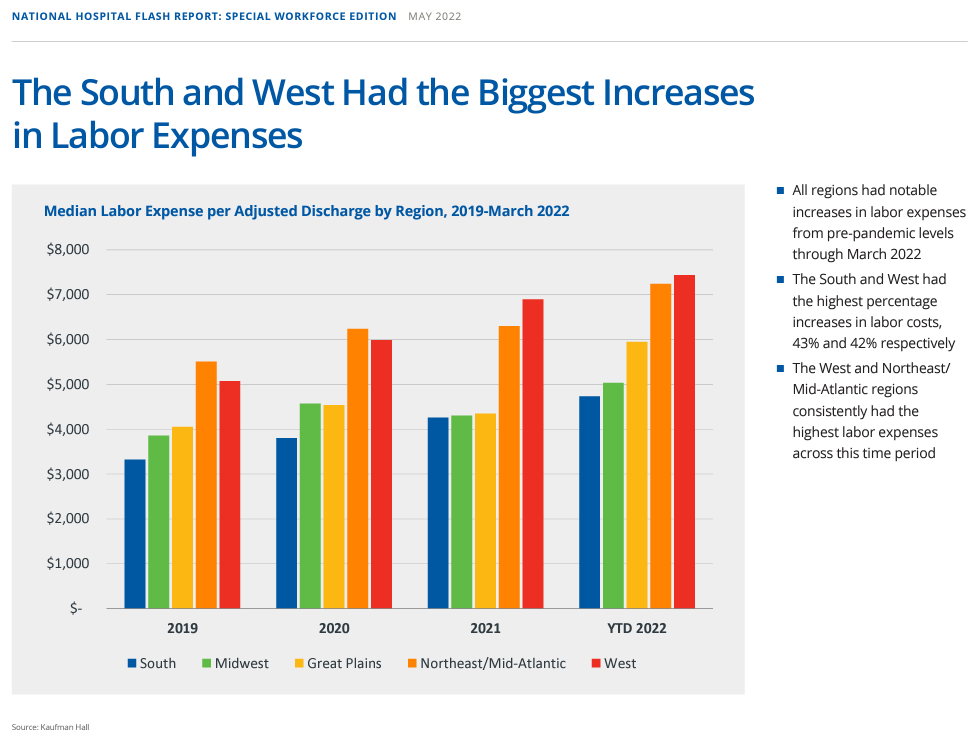
One report found that hospital labor costs rose 37% from 2019 to 2022. The same report highlighted exploding use of contract labor.

Leaving millions of Americans out of access to care threatens entrenching poorer health outcomes. Limited access to diagnostic and preventative services will likely lead to worse long-term health and lead to higher healthcare spending per patient in disadvantaged communities.
Populations with worsening health outcomes tend to be associated with higher healthcare costs. It becomes more expensive for healthcare providers to treat worsening, preventable conditions while health plans must raise premiums and deductibles to offset higher costs. It creates a vicious cycle that makes future investments in healthcare delivery less effective over time, sometimes to the extent that it deters such initiatives in the first place.
Then, of course, there is the simple market phenomenon that less healthcare professionals will drive up the price of the medical services which they provide.
What is Full Practice Authority
One proposed, but controversial, solution is to allow physician assistants (PA’s) and nurse practitioners (NP’s) to perform diagnosis, treatment, and prescriptions without the supervision of a licensed physician or agreement with the state’s Board of Medical Examiners.
Such proposals for full practice authority (FPA) would allow NPs to “evaluate patients, diagnose, order and interpret diagnostic tests and initiate and manage treatments — including prescribing medications” if the NP has a license from the state’s Board of Nursing.
In states with FPA, NPs can conduct these elements of practice. Other states have reduced practice, which allows nurses to perform at least one of these activities.

Proponents of FPA highlight reduced costs associated with NP practices and an improvement of health outcomes for areas with historically poor access to health. Through an analysis of counties along the Maryland-Pennsylvania border, implementation of FPA in Maryland greatly increased the density of NPs in Maryland counties. The same report estimated that FPA in Pennsylvania could eliminate half of the designated health professional shortage areas (HPSAs) in the state.
Another study suggested that through FPA, higher use of routine healthcare services reduced emergency room admissions from preventable concerns while reducing administrative and duplicative costs associated with physician supervision. The implication is savings for government programs like Medicare and Medicaid and even private health plans.
As indicated in the chart above, states like Montana, Wyoming, and North Dakota have already implemented FPA for nurses, and multiple bills seek to extend similar independence for PA. It is no surprise that these measures are being spearheaded by low-density states with large swaths of rural area.
Balancing Quality and Access
These measures have brought up opposition from patient safety advocates and physicians. The argument is that NPs and PAs do not receive as much training and could endanger the lives of patients.
One working paper on the National Bureau of Economic Research analyzed the relationship between NP care in the emergency department (ED) and patient outcomes. The paper found that patients getting care from NPs had stays longer in the ED by 11% and increased the cost of care by 7%. This body of research came from an analysis of 1.1 million visits to EDs from the Veterans Health Administration (VHA).
One significant argument is that allowing NPs and PAs this independence “could lead to siloed care and that team-based care is the better alternative.” Retaining the role of the physician prevents overlooking certain conditions and diagnoses whilst also having a highly trained professional ready for more complex cases.
These ongoing debates are crucial to watch, especially for those involved in consumer health and virtual care. Even if physicians against such PA and NP independence may be looking out for their own jobs, there are valid questions to ask about how consumer health tools powered by questionnaires and AI or clinicians who cannot interact with the patient’s person physically will ensure the same level of care quality.