
Six Pharma Companies are Suing the Feds
What is 340B, and why is there a huge fight about it?

Last night, President Biden gave the annual State of the Union address. Having lost control of the House of Representatives, the speech was less ambitious in calling for expansion of social spending and investments into areas like cancer, mental health, and opioid abuse. However, he stuck to his platform to leverage federal authority to rein in out of pocket healthcare costs.
Addressing some Republicans who have threatened to repeal the Inflation Reduction Act, Biden proclaimed:
Make no mistake, if you try anything to raise the cost of prescription drugs, I will veto it.
We can go on about Medicare negotiating drug prices and prescription drug price ceilings, but the court system just dealt a blow to a less talked-about federal program to expand access to drugs.
This program — the 340B Drug Pricing Program — is at the core of a huge fight between the federal government and care providers on one side, and pharmaceutical companies on the other.
Supporting Care for Low-Income Patients
Medicaid, the federal and state health program to cover low-income Americans, imposes certain requirements on pharmaceutical companies in order to have drugs covered by Medicaid plans. Because the Medicaid program covers millions of Americans (76 million in summer 2021), these drug manufacturers have a large incentive to comply with federal and state requirements to have access to this large market of patients.
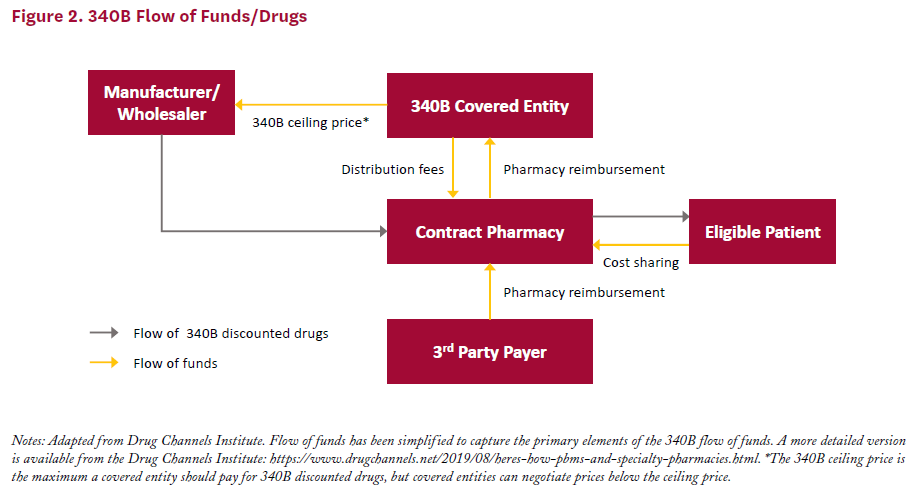
In an effort to control spending on drugs, Congress created the 340B Drug Pricing Program in 1992, named after Section 340 of the Public Health Service Act. Under 340B, pharmaceuticals have to offer discounts on the order of 25-50% for outpatient drugs sold to covered entities like certain hospitals and clinics.
In general, eligible covered entities are non-profit or government healthcare providers whose patient populations consist of a large number of low-income and disadvantaged patient groups. With these savings, safety net healthcare providers can save financial resources to treat more underserved patients.
When considering the care of low-income Americans, many of whom are uninsured, the 340B Program also assists hospitals in dealing with the cost of uncompensated care. The Emergency Medical Treatment & Labor Act (EMTALA) requires hospitals to examine, treat, or transfer all patients coming for emergency examination and treatment regardless of the patient’s ability to pay. When an uninsured patient comes into the ER, there is a chance that they will not be able to pay, and the care provided by the hospital goes uncompensated.
The American Hospital Association (AHA), a trade group of hospitals, notes that the national cost of uncompensated care was over $40 billion in each of 2018, 2019, and 2020. Savings from programs like 340B provide significant support to hospitals treating large low-income populations that correlate with higher rates of uncompensated care.
Drama and Attempts at Oversight
Of course, with any policy, there are winners and losers. In this case, pharmaceutical companies must lose out on profits. The Affordable Care Act (ACA) of 2010 expanded the definition of which organizations count as covered entities, and the usage of the 340B program exploded. Further, the ACA allowed providers to contract with any number of third-party pharmacies to dispense these drugs purchased at a discount.
Adoption of the program has exploded. In 2000, 8,100 sites were participating in the discount program, and by 2020, that number ballooned to 50,000 sites. The value of discounted purchases surpasses $40 billion annually.

Drug manufacturers argue that many of the program’s operations are not transparent and lack oversight. They claim that discounts are being duplicated, especially with contract pharmacies — demanding covered entities to submit drug claims data and not applying discounts in some cases.
The Trump and Biden administrations have been fairly consistent in asserting that covered entities are largely compliant, and that in fact, drug manufacturers are not delivering enough discounts to hospitals and providers. A December 2022 audit document found that three of five audited drugmakers did not follow price ceilings and had to repay providers. Another firm was placed on a corrective action plan to submit proper pricing data.
Another consideration to make is that in 2020, 340B-priced drugs made up only 7% of the American drug market.
Legal Battles and the Near Future
Members of Congress have not been afraid to call on the Department of Health and Human Services (HHS) to go after manufacturers more aggressively for overcharging covered entities. This includes members of both parties like Representative Abigail Spanberger (D-VA) and Senator Chuck Grassley (R-IA) who sent letters to the Biden administration to call for updates on investigations into enforcement action against pharmaceutical companies violating 340B provisions.
A number of cases are circulating in the federal court system. Remember the unlimited contract pharmacies that 340B-participating providers can work with? In summer of 2020, six pharmaceutical companies imposed restrictions on discounted drug sales to contract pharmacies. In 2021, the Health Resources and Services Administration (HRSA), which administers 340B under HHS, issued a warning on these companies — Eli Lilly, Sanofi, United Therapeutics, Novartis, AstraZeneca and Novo Nordisk — to lift restrictions or face $5,000 penalties for each violation of the 340B program.
These companies launched a flurry of lawsuits against HHS claiming that they are allowed to restrict discounts to contract pharmacies to prevent giving duplicated discounts to contract pharmacies and covered entities of the 340B program.
A few big cases have made their way to appeals courts across the federal judiciary:
DC: Novartis Pharmaceuticals v. Carole Johnson, et. al.; United Therapeutics v. Carole Johnson, et. al.

In lower courts, the messages were somewhat mixed on whether the federal government sides with pharmaceuticals or HHS’ interpretation of the 340B law. One of the first appeals cases has already been decided in the 3rd district, wherein judges sided with Sanofi, Novo Nordisk, and Astra Zeneca.
The judge ruled in late January 2023:
Congress never said that drug makers must deliver discounted Section 340B drugs to an unlimited number of contract pharmacies. So by trying to enforce that supposed requirement, the government overstepped the statute’s bounds
Drugmakers celebrate this ruling, and providers are railing against the decision. Other case decisions in the 7th and DC courts may contradict this, and these cases may work up to the Supreme Court.
In the balance are billions worth of drugs and potentially the financial survival of several care providers across the country.