
A Consumer Health Renaissance is a Far Away
The fabled utopian consumer health ecosystem requires economic realignment

It feels like every other day, I hear about a soon-to-come revolution in healthcare driven by this idea that ubiquitous computing, access to vast sums of data, and now, AI, will create person-centric care. Patients will finally be able to decouple from the nonsense of the healthcare system and see unparalleled improvements in physical and mental health.
It’s not hard to see why many want to believe this.

Health systems are bloated, bureaucratic entities where physicians are beholden to shareholders, board members, and payers more so than patients. Clinical and patient advocates must always fight claw their way into budget meetings. Independent practices are being driven out of the market by stagnant reimbursement rates and cut-throat competition with consolidated provider systems.

Things are not exactly rosy on the payer side. The public’s sympathy for Luigi Mangione across the political spectrum sent a clear message to payers that they are seen as appropriate targets of violence.

I see the promise of a consumer health renaissance among the tech community to be an innocent optimism — as in I will not assume you’re a bad person for believing it. However, these ideals are not informed by the realities of the majority (or rather a combination of pluralities of) Americans and their interactions with the healthcare system, which itself is just one aspect of each person’s life.
A revolution in Americans utilizing personalized medicine driven by direct-to-consumer apps, generative AI, and decoupling from payers and health systems is likely impossible, at least in terms of reaching more than 10% of the country under the best of conditions.
This article is my take on why this promised consumer health renaissance is not likely to happen, informed largely from my learnings traveling to rural communities, speaking with providers, administrators, and patient advocates for the past several years.
The Last Consumer Health Wave
There have been pushes for the creation and adoption of consumer health technologies before the current generative AI rush. The most recent was the 2010s when “interoperability” was the great buzzword.
The Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 and 21st Century Cures Act of 2016 were signs of federal support for digitization of medical records and adoption of standards for exchanging health information. This was accompanied by the widespread adoption of the electronic health record (EHR), standardized clinical quality measures, statewide health information exchanges, and with them, a collection of modernized data standards from HL7 and C-CDA to FHIR.
Interoperability came about as a buzz word in the industry. Patient records fragmented and often not shared between healthcare providers made for obvious concerns about patient safety and care coordination. Mandates for developer-friendly interfaces to EHRs were supposed to introduce space for health tech products to address niche clinical concerns of different patient populations and financial objectives for payers and providers.
The access to patient-level FHIR data, ubiquity of smartphones, and a consensus that interoperability is key to better medical and financial outcomes created this energy of enthusiasm. More specifically, there was a promise of digital health startups being able to leverage medical records of patients to create truly personalized experiences navigating chronic conditions, projecting future health risks, and juggling multiple providers.
Americans’ relationship with the healthcare system has not dramatically changed. A lot of that is because the adoption of such technologies by the masses are fully blocked by some harsh realities.
For one, there will always be a “digitally illiterate” subset of patients which must always be tended to. While that is around, we will not see health systems and payers fully commit to digital and consumer health paradigms of care delivery, because juggling both digital and brick-and-mortar care delivery requires more buy-in and alignment than most tech startup teams are willing to push through.
The more notable concern is that digital and consumer health adoption has a solid socioeconomic boundary. Conventional wisdom about technology adoption models a bell curve where the majority of users adopt technology at an inflection point after which there’s enough momentum to reach late adopters.

In healthcare go-to-market plans trying to reach the true mainstream (not just the tech elite), “laggards” and even much of the “late majority” do not have the capacity to take on such technology.
These are Socioeconomic Concerns
When I speak with providers in rural health clinics (RHCs), critical access hospitals (CAHs), federally qualified health centers (FQHCs), and free and charitable clinics, we must focus a great deal on what provider staff can do.
Many people in distressed communities do not have the time, energy, or education to do much more than go to follow ups and take medication.
Consider one example of patient portals connected to EHRs. Patient portal usage is rarely a focus of discussions, and expecting patients to prepare forms ahead of time is not something we can count on.
At best, there’s 20-30% of patients using patient portals, and it’s far from integrated into the patient journey. Poor access to smartphones/broadband and poor digital literacy are the primary barriers here. If you take a step back, another common challenge is patients struggling with basic literacy when completing paper intake forms in the lobby.

These problems are not exclusive to rural and safety net providers. Look at providers in urban and suburban areas. A small share of patients engage in fully digital experiences. The digital literacy and health literacy necessary to use these tools limits implementation to particularly high-income and young populations.
Personalized medicine may help patients skip expensive gatekeepers in primary care or access lower-cost drugs and alternative treatments. However, these tools are restricted to the most tech-savvy parts of American society who statistically have better educational attainment and disposable income.
Healthcare system effectiveness and efficiency is not a technology problem — it is a socioeconomic problem.
Patients with lower incomes and educational attainment across the board have less available time to learn how to engage with these types of digital health tools, have less ability to comprehend how to use these tools in the first place, and often do not have the economic means to access high-speed internet. Even without digital health tools, the poorest members of American society tend to be the sickest.

These groups of Americans may face challenges with transportation to follow-up appointments, inability to afford long-term treatment options, and may not have the know-how of engaging with health insurance programs like Medicaid. Housing instability, food insecurity, poor education, and other socioeconomic factors float to the top in personal concerns and often prevent patients from being able to pursue practices that should yield long-term positive health outcomes.
Encouraging personal responsibility is not a serious policy fix.
Expecting patients to follow best-practices simply because it is the responsible thing to do is not a practical solution. Someone’s decision to adhere to treatment plans or learn to use digital health tools will be a function of their health literacy and other personal priorities for well-being.
Health literacy is built through strong social support systems and educational institutions. Against the backdrop of public education systems being gutted and the vilification of public health education programs, broader economic trends can help illustrate why even Americans growing up in middle-class lifestyles are less likely to prioritize health-related activities to an extent required to make personalized digital health tools useful.
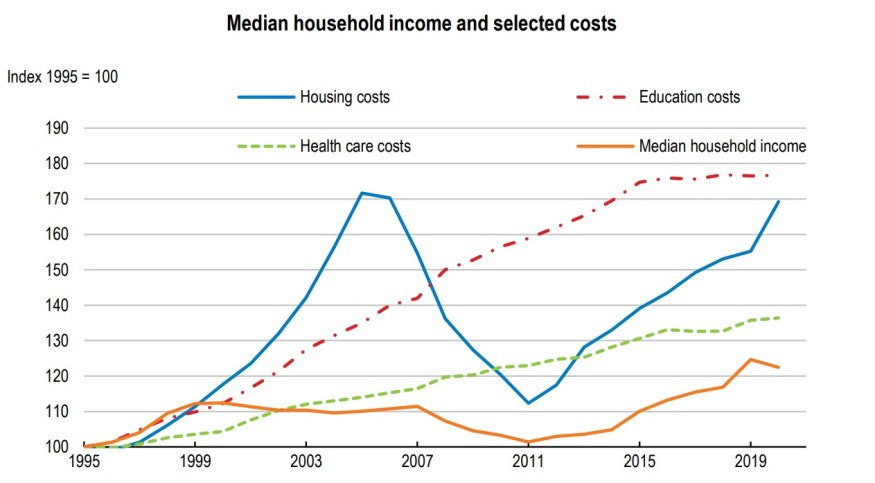
The cost burdens of education, housing, and health have far outpaced growth in wages adjusted for inflation. This is a trend unfolding for decades. More Americans of the bottom three quintiles are barely hanging on.
In what little time remains after meeting career and family obligations, it’s only logical to assume a person would rather prioritize recreation (or doing nothing to prevent incurring additional costs) than learning or updating a digital health tool.
To most Americans, the long-term benefits of most consumer health tools are marginal at best, especially if at the end of the day, you still need to engage with a physician to get a physical treatment or prescription.
In other words, to the average American, digital health tools are cool in theory but not useful enough to integrate into daily life.
What would make personalized medicine work
This is not to say that mass adoption in personalized medicine that legitimately improves health outcomes is impossible. However, it does require serious economic realignment that bucks the trend of the past 50 years.
The following requirements are deeply interconnected with each other. Yes, this is quite a laundry list, especially one to push through state legislatures and federal policy. But this illustrates the scope of problems which technology alone will not fix in an effort to consumerize healthcare.
Health System Simplification
In the context of developing systems for patient referrals, health information exchange, and facilitating addressing of social needs, complexity is driven by market and regulatory fragmentation.
Some concerns which have to be addressed in no particular order through policy (no, overpriced SaaS won’t fix this):
Consistency in licensing and credentialing processes across state lines — ideally allowing clinicians to more easily practice across state lines
Standardized utilization management protocols and enforceable rules for timeliness and preciseness of payer responses
Technical assistance to train staff at understaffed state-level public health agencies and greater funding accompanied by stronger mandates for ending healthcare deserts
Expansion of the clinical workforce through grants to pursue education and pressure on educational institutions to stop coast bloat (consumer health will still require physicians for hand off and signing orders)
Strong reimbursement for social work and efforts to connect patients to housing, food, and education as part of the continuity of care
Reinvesting in Education:
There is a core belief in the American psyche that government services are inherently inferior to those of the private markets. This is a stance which I strongly disagree with — it is a self-fulfilling prophecy and policy choice to throw hands up and say public education cannot be salvaged. This does not have to be a liberal stance. Notably, rural Republican Texas legislators recognize the reliable economic anchor that robust public education is.
Just like healthcare, educational attainment exists among a person’s other socioeconomic needs. Weak household wage growth, poor nutrition, and lack of access to reliable housing will make someone less able to make advances in education.
However, well-supported educational systems pay for themselves multiple times over. As it relates to personal medicine, strong public education institutions particularly help low and middle-income students in literacy (general, digital, and health) and development of social support systems. They also greatly improve social mobility by opening opportunities to higher-skill and better paying jobs.
The long-term economic benefits as well as immediate improvements to literacy would enable more patients to meaningfully engage with consumer health apps and know the value of consistent efforts to improve long-term personal health through lifestyle choices.
True Interoperability
There will always need to be a handoff between personalized and traditional delivery of medicine. This means the bidirectional exchange of health information so that personalized apps can have the context necessary to operate while also having the means to share data back to a referred provider.
One of the great challenges with interoperability is the need for health IT systems to be robust. Each EHR vendor must do its best to ensure that excessive data is not shared outside of its network with untrusted entities while also making sure that data ingested from outside partners is valid. Every provider having different instances of EHR products using a variety of tools faces a similarly dizzying number of custom integrations to pay for.
As long as there are different provider entities using an array of potential EHRs, this challenge of the consistency of data integration approaches and costs will persist. We can talk about solutions like TEFCA, but even that’s limited when considering that each EHR has its own feature set and that a truly universal data exchange framework may not be easy to integrate with EHRs lacking certain features.
Creating an extensive minimum set of requirements for national-level interoperability is a beast in and of itself. Not only does this greatly expand the scope of work required by EHR developers, but it would likely create a prohibitive barrier to entry for smaller EHR vendors to build their presence in niche provider specialties and use cases.
The key here is striking that balance wherein new entrants to the EHR market are not blocked from competing with incumbents while ensuring there is enough nationwide consistency for consumer health developers to facilitate the patient data handoff securely and effortlessly across the country.
Robust Social Mobility
There is a great expectation of patients in consumer health models to be proactive to their health. The assumption is that with the promise of better health in the future, patients are more likely to comply with treatment plans and regularly engage with digital health tools.
One of the pitfalls of this assumption is that demonstrated outcomes are not enough to motivate a person to pursue what may be the “best practice”. The personal locus of control, a person’s belief of how much individual decisions impact outcomes compared to external influences, is a key aspect of whether someone will adhere to a self-managed and personalized plan. This is true of chronic disease management, fitness and diet, education, career growth, and personal finance. (Some reading)
Someone with an external locus of control will feel as though their own actions will not overcome the power of institutions, macro trends, and even other personal authority figures in determining the outcome of life events. Much of the literature around locus of control suggests that those with an internal locus of control have greater social mobility and health outcomes (driven by higher incomes, better education, and healthy lifestyles).
However, an internal locus of control, which is necessary for someone to believe personal health activities should be pursued regularly, is largely conditioned. Stagnant wage growth relative to productivity, ballooning costs of living, and the erosion of affordable public services have led to a collapse in social mobility.

It is no wonder that (especially among younger generations), Americans are growing more apathetic or outright pessimistic, not only about the state of the country as a whole, but also personal future outcomes. The despair about affording the cost of health insurance (which doesn’t even cover many services), being able to retire, or have time to enjoy even personal hobbies is likely to not bode well for the adoption of consumer health apps by startups claiming to have the singular answer to peoples’ problems with a monthly subscription.
Fixing social mobility would be quite an array of policy implementations. It would mean the revitalization of entire cities, improvements in public health and education, revival of small business, anti-trust and enforcement of corporate abuse, and a politics of abundance which control the cost of living.